Overview
 A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.
A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.
Causes
The Achilles tendon is a strong bands of fibrous connective tissue that attaches the calf muscle to the heel bone. When the muscle contracts, the tendon transmits the power of this contraction to the heel bone, producing movement. The Achilles tendon ruptures because the load applied to it is greater than the tendon's ability to withstand that load. This usually occurs as a result of a sudden, quick movement where there is a forceful stretch of the tendon or a contraction of the muscles eg: jumping, sprinting, or pushing off to serve in tennis. This occurs most often in sports that require a lot of stopping and starting (acceleration-deceleration sports) such as tennis, basketball, netball and squash. The Achilles tendon is on average 15cm in length. Most ruptures occur 2-6cm above where the tendon inserts into the heel bone. This is the narrowest portion of the Achilles tendon and is also the area with the poorest blood supply. achilles tendon rupture is most common when the muscles and tendon have not been adequately stretched and warmed up prior to exercise, or when the muscles are fatigued. the Achilles tendon has a poor blood supply, which makes it susceptible to injury and slow to heal after injury. During exercise the amount of blood able to travel to the tendon is decreased, further increasing the risk of rupture. Most experts agree that there are no warning signs of an impending rupture. However, frequent episodes of Achilles tendonitis (tendon inflammation) can weaken the tendon and make it more susceptible to rupture.
Symptoms
The classic sign of an Achilles' tendon rupture is a short sharp pain in the Achilles' area, which is sometimes accompanied by a snapping sound as the tendon ruptures. The pain usually subsides relatively quickly into an aching sensation. Other signs that are likely to be present subsequent to a rupture are the inability to stand on tiptoe, inability to push the foot off the ground properly resulting in a flat footed walk. With complete tears it may be possible to feel the two ends of tendon where it has snapped, however swelling to the area may mean this is impossible.
Diagnosis
The diagnosis of an Achilles tendon rupture is made entirely on physical examination. Often, there is a substantial defect in the Achilles from 2-5 cm before it inserts into the heel bone. However, the main test is to determine whether the Achilles has been ruptured is the Thompson test. This essentially involves placing the patient on their stomach and squeezing the calf muscle. If the Achilles is intact, the foot will rise [plantar flex]. If it is ruptured, the foot will not move and will tend to be in a lower lying position.
Non Surgical Treatment
Not every torn Achilles tendon needs an operation. Recent studies have shown that even a conservative treatment, i.e. immobilizingt the leg can lead to satisfactory healing successes. This requires, however, that the patient is fitted with a cast (immobilization splint) and/or a special boot for a period of approximately 6 - 8 weeks. After that, the boot must be worn during the day for about two more weeks. An intensive physiotherapy will start after about six weeks to train the calf muscles so that the initial coordination can be restored. Running training on flat ground can be started again after another 10 - 12 weeks. Studies show that the danger of a recurring torn tendon is higher after a conservative treatment opposed to an operative treatment. Depending on the type of treatment, about 10 - 15 percent of those affected can expect at some point to again suffer from a tear of the Achilles tendon. Moreover, in the non-operated cases, we see more often a significant permanent weakness of the footprint, particularly restricting the ability to participate in sports.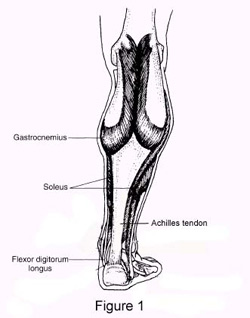
Surgical Treatment
The goal of surgery is to realign the two ends of the ruptured tendon to allow healing. There are multiple techniques to accomplish this goal that will vary from surgeon to surgeon. Recovery from this injury is usually very successful with return to full function in approximately 6 months. Post operatively casting is required with the use of crutches or other means to remain non-weightbearing for 4-8 weeks. This is followed by a course of physical therapy. Partial rupture may or may not require surgical intervention depending on the extent of injury but cast immobilization is a common requirement.
A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.Causes
The Achilles tendon is a strong bands of fibrous connective tissue that attaches the calf muscle to the heel bone. When the muscle contracts, the tendon transmits the power of this contraction to the heel bone, producing movement. The Achilles tendon ruptures because the load applied to it is greater than the tendon's ability to withstand that load. This usually occurs as a result of a sudden, quick movement where there is a forceful stretch of the tendon or a contraction of the muscles eg: jumping, sprinting, or pushing off to serve in tennis. This occurs most often in sports that require a lot of stopping and starting (acceleration-deceleration sports) such as tennis, basketball, netball and squash. The Achilles tendon is on average 15cm in length. Most ruptures occur 2-6cm above where the tendon inserts into the heel bone. This is the narrowest portion of the Achilles tendon and is also the area with the poorest blood supply. achilles tendon rupture is most common when the muscles and tendon have not been adequately stretched and warmed up prior to exercise, or when the muscles are fatigued. the Achilles tendon has a poor blood supply, which makes it susceptible to injury and slow to heal after injury. During exercise the amount of blood able to travel to the tendon is decreased, further increasing the risk of rupture. Most experts agree that there are no warning signs of an impending rupture. However, frequent episodes of Achilles tendonitis (tendon inflammation) can weaken the tendon and make it more susceptible to rupture.
Symptoms
The classic sign of an Achilles' tendon rupture is a short sharp pain in the Achilles' area, which is sometimes accompanied by a snapping sound as the tendon ruptures. The pain usually subsides relatively quickly into an aching sensation. Other signs that are likely to be present subsequent to a rupture are the inability to stand on tiptoe, inability to push the foot off the ground properly resulting in a flat footed walk. With complete tears it may be possible to feel the two ends of tendon where it has snapped, however swelling to the area may mean this is impossible.
Diagnosis
The diagnosis of an Achilles tendon rupture is made entirely on physical examination. Often, there is a substantial defect in the Achilles from 2-5 cm before it inserts into the heel bone. However, the main test is to determine whether the Achilles has been ruptured is the Thompson test. This essentially involves placing the patient on their stomach and squeezing the calf muscle. If the Achilles is intact, the foot will rise [plantar flex]. If it is ruptured, the foot will not move and will tend to be in a lower lying position.
Non Surgical Treatment
Not every torn Achilles tendon needs an operation. Recent studies have shown that even a conservative treatment, i.e. immobilizingt the leg can lead to satisfactory healing successes. This requires, however, that the patient is fitted with a cast (immobilization splint) and/or a special boot for a period of approximately 6 - 8 weeks. After that, the boot must be worn during the day for about two more weeks. An intensive physiotherapy will start after about six weeks to train the calf muscles so that the initial coordination can be restored. Running training on flat ground can be started again after another 10 - 12 weeks. Studies show that the danger of a recurring torn tendon is higher after a conservative treatment opposed to an operative treatment. Depending on the type of treatment, about 10 - 15 percent of those affected can expect at some point to again suffer from a tear of the Achilles tendon. Moreover, in the non-operated cases, we see more often a significant permanent weakness of the footprint, particularly restricting the ability to participate in sports.
Surgical Treatment
The goal of surgery is to realign the two ends of the ruptured tendon to allow healing. There are multiple techniques to accomplish this goal that will vary from surgeon to surgeon. Recovery from this injury is usually very successful with return to full function in approximately 6 months. Post operatively casting is required with the use of crutches or other means to remain non-weightbearing for 4-8 weeks. This is followed by a course of physical therapy. Partial rupture may or may not require surgical intervention depending on the extent of injury but cast immobilization is a common requirement.
